
Author: Anja Henner, PhD, Principal Lecturer (emerita)
Mammography has been one form of imaging performed in Finland since the 1970s. There has been a great change and development in how images are stored: from paper printouts to X-ray film to digital in just over five decades. However, the current generation of radiographers, radiologists or physicists probably do not remember single emulsion film, the slowed down speed of the film processing machine, or the raised temperature of the developer, not to mention the precise quality control of the entire process. Here are a few highlights from the past to the present.
Background
The story goes that the first idea for mammography came in Rochester in 1924, when a group of radiographers, presumably men, admired the chest X-ray of a presumably large-breasted woman on an illuminator. While looking at the image, they playfully and seriously wondered if tumors could be detected in a breast with X-rays. What is known for certain is that German surgeon Albert Salomon took X-rays of removed breasts in 1913 to show the spread of cancer to the lymph nodes in the armpit. Salomon was also able to distinguish between local, limited breast cancer from cancer that had spread to tissues based on an X-ray image. Mammography was introduced to living patients when the American Stafford L. Warren presented in his article published in 1930 how important it is to compare the image of both breasts side by side, and how reliable mammography is as an imaging method: Out of 119 people’s images, only eight cases were misinterpreted. The Uruguayan radiologist Raul Leborgne introduced the importance of compression in mammography in 1949, and after that Gershon-Cohen discovered the importance of breast compression for improving the quality of mammography. After these research results, people were convinced of the benefits of mammography and an increasingly wider group of people were attracted to the development of the technology. However, the rapid development of mammography did not happen until the 1970s.
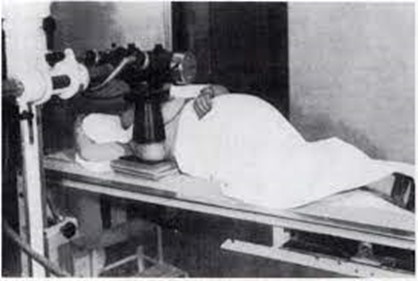
The first steps in mammography were actually taken in the 1950s (image 1953, Leborge); we can only guess how diagnostic the image might have been and what kind of radiation doses the image was created. According to some estimates, the dose from one mammography examination was as much as 1-2 rad. (1 Gy = 100 rad)
Breast cancer screening as part of the healthcare system
In America, an extensive study was conducted in 1963-1966 aimed at demonstrating the benefit of mammography in the early detection of cancer. Breast cancer screening received further confirmation in 1974, when Myron Moskowitz and his associates introduced new research material, and the final confirmation of its benefits emerged in the 1980s. An important researcher and developer is Swedish László Tabár, who is familiar to the older generation of people involved in X-rays. He has conducted a lot of research and trained and taught in different countries about the importance of mammography screening since 1985, when he presented 134,867 women (age range 40 – 79 years) with a 31% reduction in breast cancer mortality thanks to early detection based on an oblique view of a single breast. Screenings in Finland started in 1987, and under the Public Health Decree (1992), municipalities were required to provide free screening every two years for women aged 50-59. Nowadays, screening is done for 50-69 year olds.
The modern era of mammography began in the 1970s
The 1970s is called the modern era of mammography; perhaps today the modern era could be moved up to the 21st century. Although the man called the father of mammography, Robert L. Egan, had introduced a fine grain intensifying screen and commercial film to improve image quality as early as the 1950s, it was not until the 1960s that special mammography devices and equipment intended for breast imaging were designed. In 1965 Charles Gross of France introduced a device with molybdenum as anode material, with a focal spot of 0.7 mm and a compression device. This achieved a high differential contrast between parenchyma, fat and microcalcifications. The importance of low imaging voltage and high current for improving image quality was also observed. In the early days, images were evaluated on paper, later X-ray film placed in light-tight cases was also used. Kauko Karila, who worked as an inspector at the Radiation and Nuclear Safety Authority, wrote in the 1/1980 issue of the Röntgenhoitaja publication: “The use of intensifying screen-film combinations should be increased in mammography, because the transition from X-ray film in light-tight cases to intensifying screens reduces doses to a level that is 1/3 to 1/30”.
In the 1970s and 1980s, equipment manufacturers operating in the field invested in the development of mammography films and intensifying screens as well as the development process. Sickles, Kunio Doi and Genant began using magnification in filming in 1977, and this required its own tools. As both clinical and screening mammography expanded in the 1980s, mammography machines, image storage, development, and dictation changed rapidly.
Cassettes, films and intensifying screens used in mammography
There was a variety of x-ray films and cassettes for mammography on the market. The X-ray film used in mammography changed from double-emulsion to single-emulsion, and instead of two intensifying screens, the X-ray cassette had only one intensifying screen, which is on the back cover for most manufacturers. The intensifying screen was fine-grained (small crystals). The aim was to get back the reflection (crossover) as small as possible and the small details of the object to be accurate. However, small crystals produced less light, requiring more radiation. The X-ray film used in mammography was sharp, so the exposure latitude was small. This combination revealed small details and small differences in the density of tissue. However, the slow intensifying screen required a larger radiation dose, and the sharpness of the film required the precisely correct radiation dose. Because of this, mammography devices came with an automatic exposure control (AEC) at an early stage; this measured the amount of radiation that passed through the breast in order to achieve the correct density of the image. In skeletal X-rays, the automatic exposure control could be adjusted in three steps in each direction, but in the mammography device there were up to seven steps in each direction. In the mammography machine, the automatic exposure control was located below the cassette, to prevent the measuring chamber from being visible in the image (above the cassette in skeletal imaging). Normally, there is a thin lead sheet on the back cover of the cassette, but lead was not allowed in the back cover of a mammography cassette precisely because of the automatic exposure control. There were also other special requirements for the cassette: the front edge had to be as thin as possible (chest wall distance), the cassette had to be light-tight, it had to absorb as little radiation as possible and be easy to clean.

X-ray image archive before the direct digital era. (image: A. Henner)
Development of mammogram film
In the darkroom, the developer had to put the film into the cassette facing the right direction, i.e. the emulsion side of the film against the intensifying screen. The radiographic density of the film could still be “adjusted” in the developing machine by slowing down the development process of the film (normally 1.5 minutes, 3.5 minutes with mammography) and raising the temperature of the developer by a degree or two. All of this required either two different developing machines or adapting the development process between the two, while maintaining the balance between image quality and radiation dose to the patient.
Mammography in the digital age: Full-Field Digital Mammography FFDM
Mammography is probably the last imaging process to be digitized. In 1996, the Food and Drug Administration (FDA) issued guidelines for equipment suppliers on the testing and approval process for digital mammography. The first digital mammography device approved by the FDA was General Electric’s Senographe 2000 D in the early 2000s. Radiologists switched to using imaging plates for skeletal X-rays in the 1990s, and to so-called direct digital, i.e. detector-based imaging, in the 2000s. The first sufficiently precise digital CR image readers and imaging plates for mammography came in 1997 to 2000 from Fuji, Agfa and Kodak (now Carestream). The dose level did not decrease much compared to imaging on X-ray film.
At the same time, mammography equipment manufacturers developed direct digital detectors, with creates an image directly in digital format and can be stored in DICOM format in the PACS system for further viewing. Techniques have also been developed for to digitizing existing CR imaging plate-based mammography devices, so the entire device does not need to be replaced.
Tomosynthesis, or 3D mammography, ultrasound and MRI have developed tremendously in recent years. Nevertheless, traditional mammography will probably continue to be used, especially in screening, though in direct digital form.
Mammography today
The development of breast cancer research and mammography screening has been enormous in the past decades. The benefits of systematic screening are undeniable. More than 5,000 breast cancers are detected in Finland each year, most of which can be cured. Breast cancer mortality is low precisely because of effective screening.
Imaging technology has developed, and today it is increasingly direct digital. As a result, performing mammograms is easier for radiographers, and it no longer requires processing of imaging plates and films. Radiologists can be provided with even better quality images thanks to advanced detector technologies and image processing. To protect the customer against radiation, increasingly higher quality images can be obtained with even lower radiation doses. The development is going in the right direction, but there is still a lot to do.
New detector technologies and advanced image processing algorithms are introducing new dimensions to breast cancer research; one day this will also apply to screening. Increasingly smaller changes in breast tissue can be distinguished from healthy tissue. AI-assisted analysis software is also coming. Furthermore, multimodal imaging techniques, which combine different imaging technologies such as angiography and tomosynthesis, are also coming.
The development of technology in cooperation with clinical experts is a good sign for current and future generations.

Today, there are also direct digital solutions on the market that can be used to digitize existing analog mammography devices (Image of FeniX digitalization solution developed by Innomentarium Oy).
Sources:
Own notes
Röntgenhoitaja 1/1980 publication
Nitida Mekasut (2011) Mammography: From Past to Present.
Steen & Van Tiggelen Short history of mammography: a Belgian perspective. https://www.researchgate.net/publication/6143668_Short_history_of_mammography_a_Belgian_perspective
More information on new breast imaging methods http://earlydetectionofbreastcancer.weebly.com/module-3.html